

Prostate matters is a not for profit organisation committed to providing free information about prostate issues from leading Clinical Authorities

Prostate cancer treatment – high and low dose brachytherapy
Consultant Urological Surgeon, Guy’s and St Thomas’ NHS Foundation Trust

Prostate Cancer Treatment – Low Dose Rate Brachytherapy
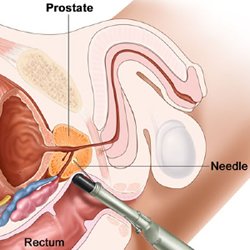
Brachytherapy is a bespoke form of radiotherapy in which delivery of radiation is targeted directly to the prostate gland by implanting small radioactive seeds under ultrasound guidance. Needles are inserted through the skin of the perineum. These needles are used to deliver the titanium seeds impregnated with radioactive material, most usually radioactive iodine. The individual seed positions can be planned very accurately with computer software to maximise the dose to the prostate whilst minimising the dose to the urethra or the rectal wall. The computer software systems can be used to optimise the dose to the most affected part of the prostate, as a “Focused” Brachytherapy implant.
Brachytherapy is carried out as a day case procedure under a light general anaesthetic.
The procedure is usually carried out by a Urologist or a Uro-Radiologist and a Radiation Oncologist supported by a physicist. Brachytherapy treatments started in the late 80s and the outcomes reported at 10 – 15 years are equivalent to standard radiotherapy and surgery. With advent of specialised MRI scanning and better targeted prostate biopsies Brachytherapy has become a highly refined and targeted prostate cancer treatment with little risk of incontinence and good preservation of erectile function.
Brachytherapy may be used as a primary therapy (monotherapy) or in combination with external beam radiation (EBRT) and or hormonal therapy dependant on disease risk.
Patient Selection:
The ideal patient for brachytherapy should have no significant urinary symptoms (IPSS < 10), a normal urinary flow rate and a prostate volume < 60 cc. Brachytherapy is not suitable for patients with large prostates (> 60cc) because the pubic arch which sits in front of the prostate may obstruct the access of brachytherapy needles to the prostate gland.
A previous transurethral resection of the prostate is not a contraindication, but it will be necessary to document a urinary flow rate and carry out a cystoscopy to assess the prostate cavity.
Some patients who have urinary symptoms (IPSS 10 -20) related to benign prostate enlargement may benefit from a transurethral resection of prostate tissue to make them more suitable for brachytherapy. The brachytherapy implant is deferred for 4 – 6 months and so these patients should have low to intermediate risk disease and be suitable for Active Surveillance.
Low to Intermediate Risk Disease Gleason 3+3 or 3+4, ISUP Group 1 – 2.
Patients considered suitable for LDR brachytherapy as a mono treatment (single visit day-case procedure) normally have a PSA <10 ug/l, a Gleason score of 6 or 7 (ISUP Grade 1 – 2), with organ confined prostate cancer, stage of T1-T2a but multifocal disease such that they are not suitable for focal therapy but can still benefit from a less invasive treatment option.
Focal Gleason 4+3 (ISUP Grade) confined to one quadrant may be suitable for a “Focused” brachytherapy implant in which the radiation dose is boosted to a very high level to maximise the dose to the involved quadrant whilst maintaining an overall standard treatment dose to the whole gland and avoiding
Intermediate to High Risk Disease (Gleason score 4+3 or even 4+4, ISUP Grade 3 – 4
You may still be considered suitable for brachytherapy but this would likely be in combination with external beam radiotherapy, If you have higher grade disease and volume of disease, including up to T3a disease and PSA is over 10, this combination treatment will often be combined with a minimum of 24 – 36 months hormonal therapy for high volume high grade disease.
Low Dose Rate Brachytherapy (LDR)
The seeds used for LDR brachytherapy give off a low dose of radiation over 6 months, remaining in the prostate gland permanently, but inactive. This does no harm
Brachytherapy in combination with a rectal spacer (SpaceOAR)
Brachytherapy can be combined with the insertion of a rectal spacer, such as SpaceOAR. This is placed at the end of the brachytherapy procedure and involves the placement of an access needle in to the fat filled space between the prostate and rectum. The two components of the SpaceOAR solution are injected together and immediately coalesce to form a gel matrix which separate the prostate from the rectum. This reduces the overall radiation dose effect to the rectal wall.
High Dose Rate Brachytherapy (HDR)
In HDR brachytherapy thin plastic catheters are inserted through a template (the same as used for template guided biopsy), through the perineal skin, and into the prostate gland. Radioactive seeds are then inserted into each catheter. A computer controls the length of time the seeds deliver radiation to the prostate through the catheter. After treatment the catheters are pulled out, leaving no radioactive material in the prostate gland. Although the treatments can be delivered in one day patients are often in hospital for two days.
Advantages of brachytherapy treatment
- Cure rates in low risk patients are equivalent to surgery or External Beam Radiation Therapy (EBRT)
- For intermediate and high risk patients, when combined with EBRT cure rates are better than for surgery or EBRT alone.
- The procedure is carried out as a day case and there is no need for a catheter
- No incisions or stitches are required
- Minimal, if any, post operative pain
- Incontinence rates are less than 1%
- Normal tissues nearby may receive a smaller dose of radiation compared with treatment with external beam radiotherapy, and therefore are less likely to be damaged.
- Recovery is quick, which means you can return to your normal activities within a few days.
Disadvantages of brachytherapy treatment
- The most common side effect is temporary urinary irritation including frequency and urgency. These symptoms will last from a few weeks to a few months and are helped by medications, such as alpha blockers.
- It may be some time before you will know whether the treatment has been successful. The PSA is checked every 6 months and it can fluctuate in the first 18 months (PSA bounce). A PSA bounce occurs more commonly in younger men and is often a sign that the treatment is having an effect on the prostate cells, generally by 3 years the PSA is at a very low level.
- With LDR brachytherapy the radioactive seeds stay inside the body permanently and emit radiation for 6 months but after they are inert and cause no problems.
- With LDR brachytherapy it is possible that individual seeds may move out of the prostate to elsewhere in the body or you may pass them in the urine, but because the dose emitted by an individual seed is so low this causes no harm and does not affect the overall treatment.
- HDR brachytherapy may require more than one radiation treatment so you may need to stay in bed for at least six hours between treatments with the tubes in your prostate. Some men find this uncomfortable and you may need to stay in hospital overnight for HDR treatments.
LDR is not currently available through the public system in New Zealand, but is available through private in most centres. If you have any comments as to how high and low dose brachytherapy content can be improved, please contact us.
Prostate matters is a not for profit organisation that is committed to providing free expert advice about prostate issues from leading Clinical Authorities
PROSTATE MATTERS
FOLLOW US
Copyright Disclaimer: We try to acknowledge copyright as appropriate. If we have used something without acknowledging copyright, this is inadvertent. Please let us know by emailing info@prostatematters.co.uk
Site design and technical development by Webtoys | Intelligent Digital Media